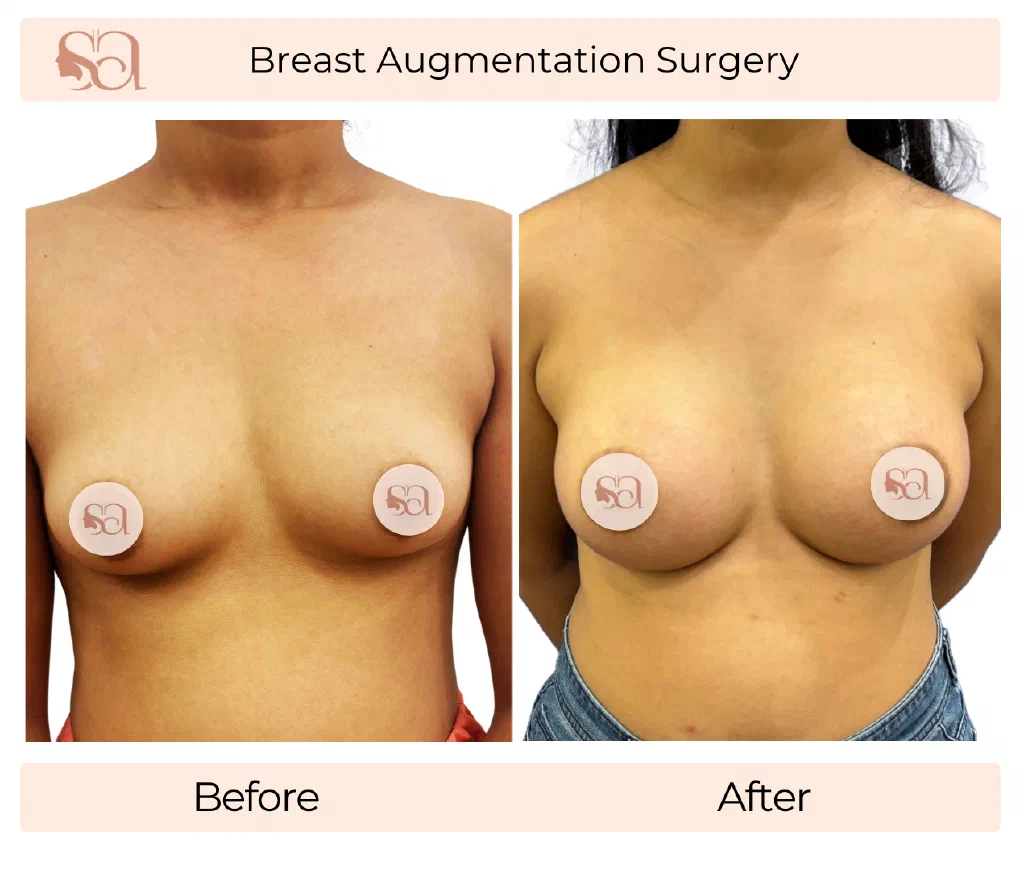
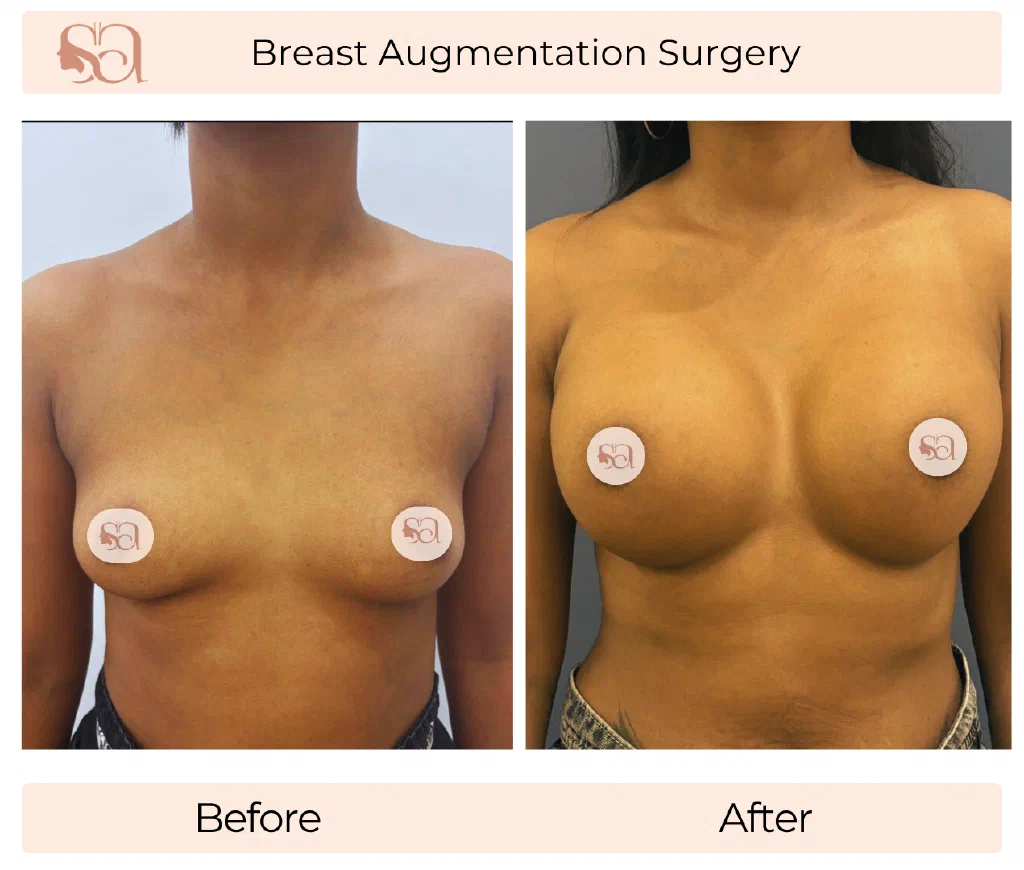
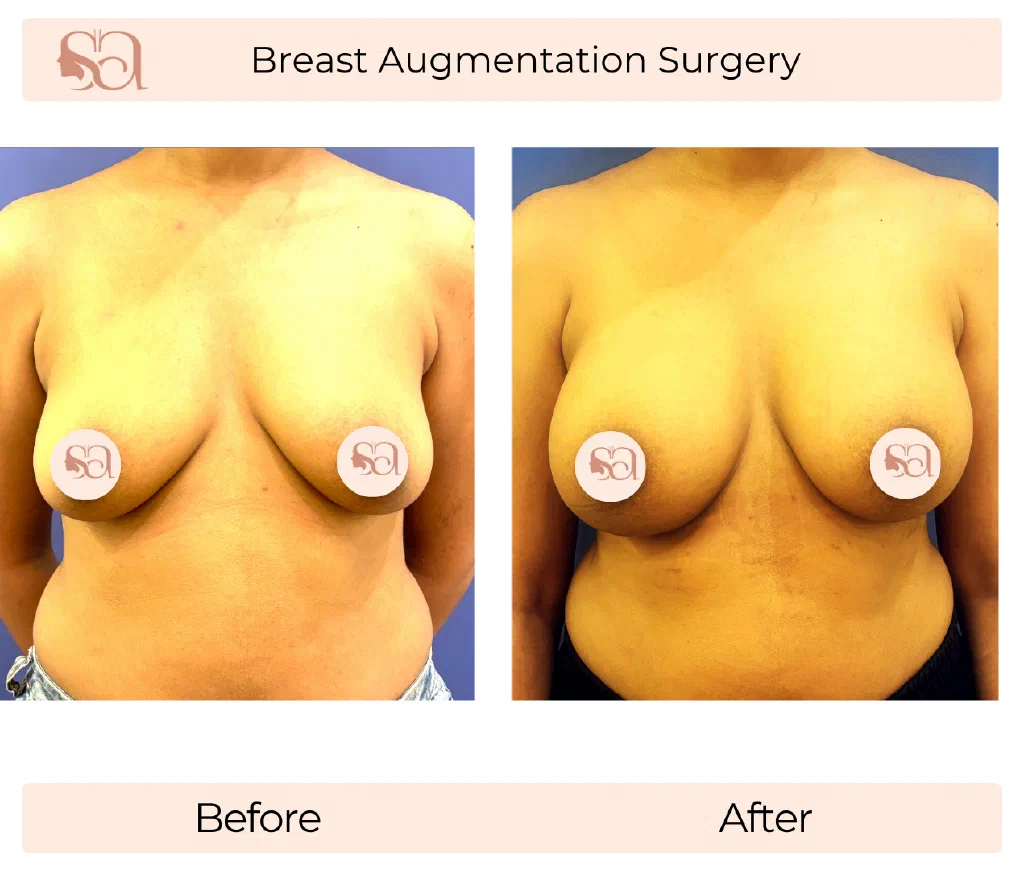
Breast augmentation — augmentation mammoplasty — is a surgical procedure that adds volume to the breast using a silicone implant, a saline implant, autologous fat transferred from another part of the body, or a combination of an implant with fat layered on top to soften the upper pole. It is the right call when the breast is genuinely small for the chest frame, has lost volume after pregnancy or weight loss, or is asymmetric in size or shape between the two sides.
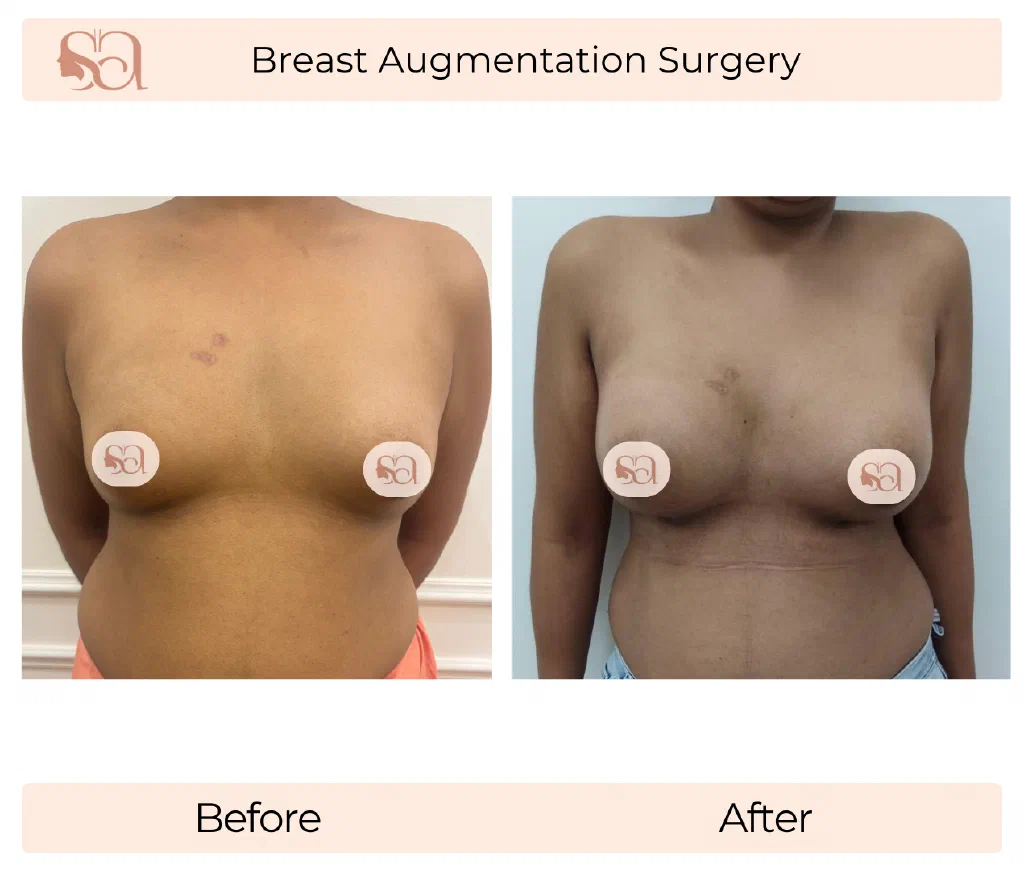
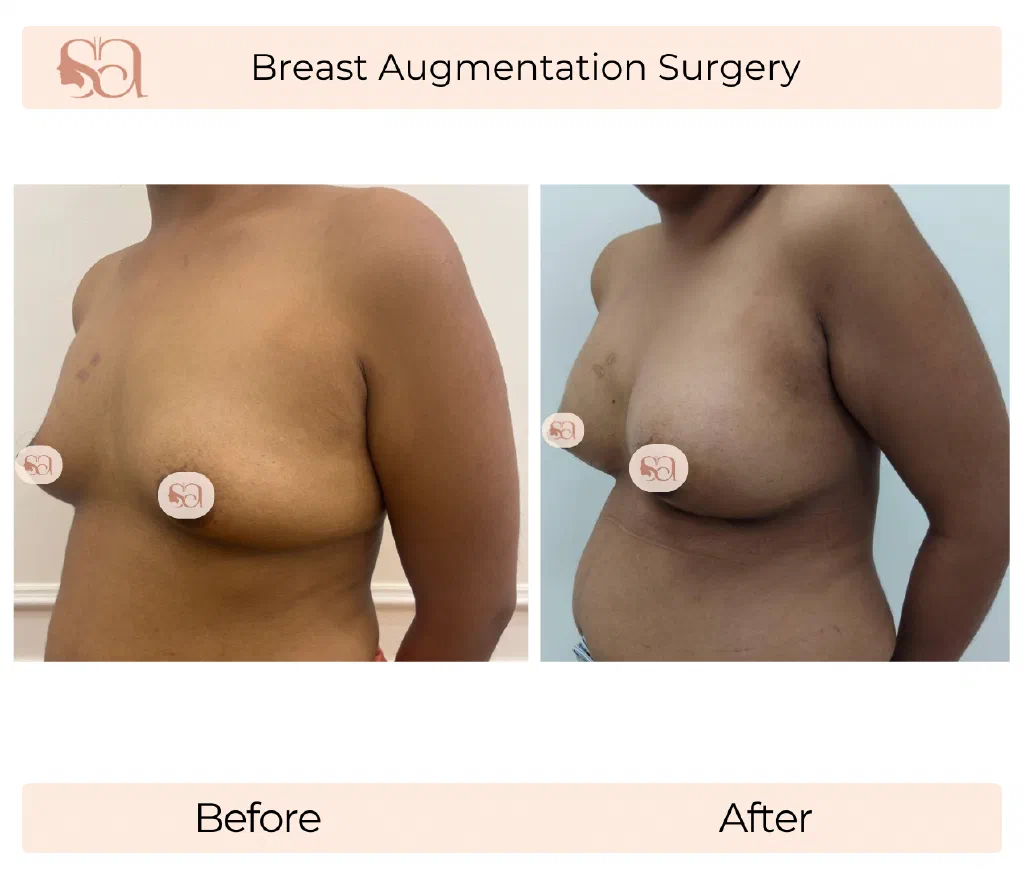
It is not a treatment for sag. When the nipple sits at or below the inframammary fold and the upper pole is hollow, the underlying problem is ptosis (drooping) of the breast tissue on the chest wall, and an implant alone cannot lift that tissue. In those cases the right plan is either a breast lift (mastopexy) on its own or an augmentation-mastopexy combined procedure — the lift addresses position, the implant addresses volume. The candidacy decision between augmentation, lift, and the combined operation is a recurring conversation in the Gurgaon practice, and the clinically related options are discussed on the breast lift in Gurgaon page.
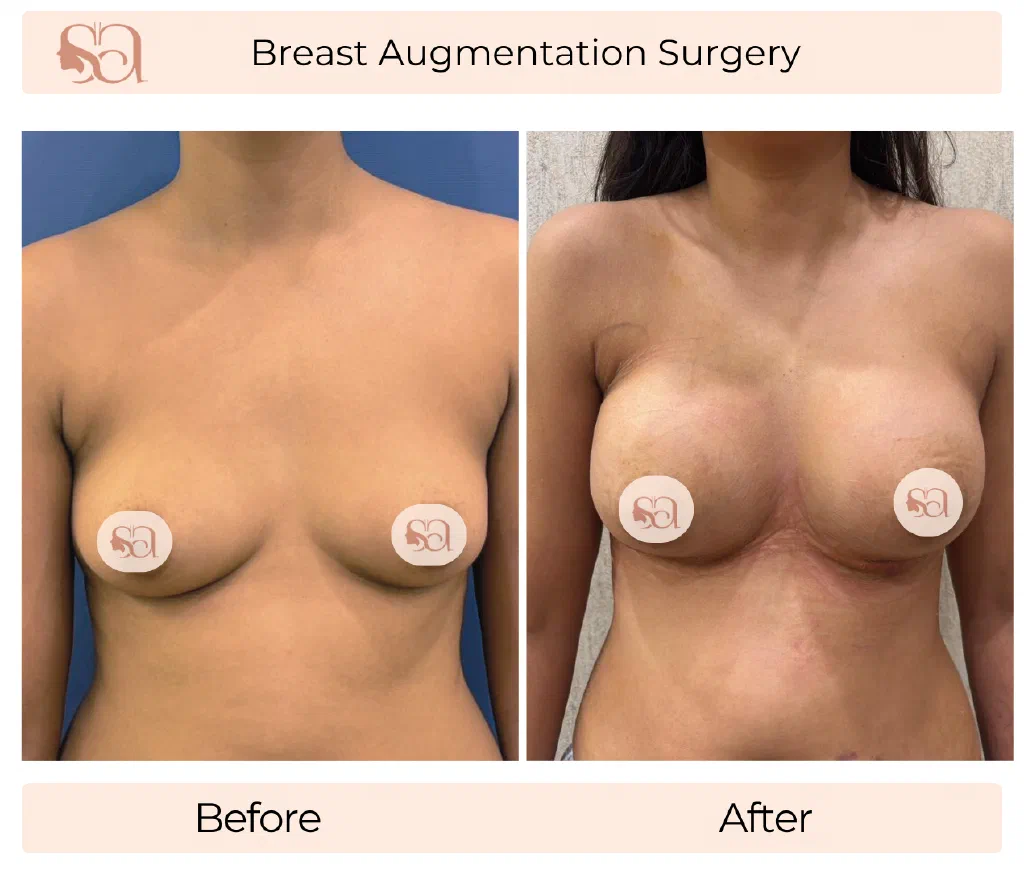
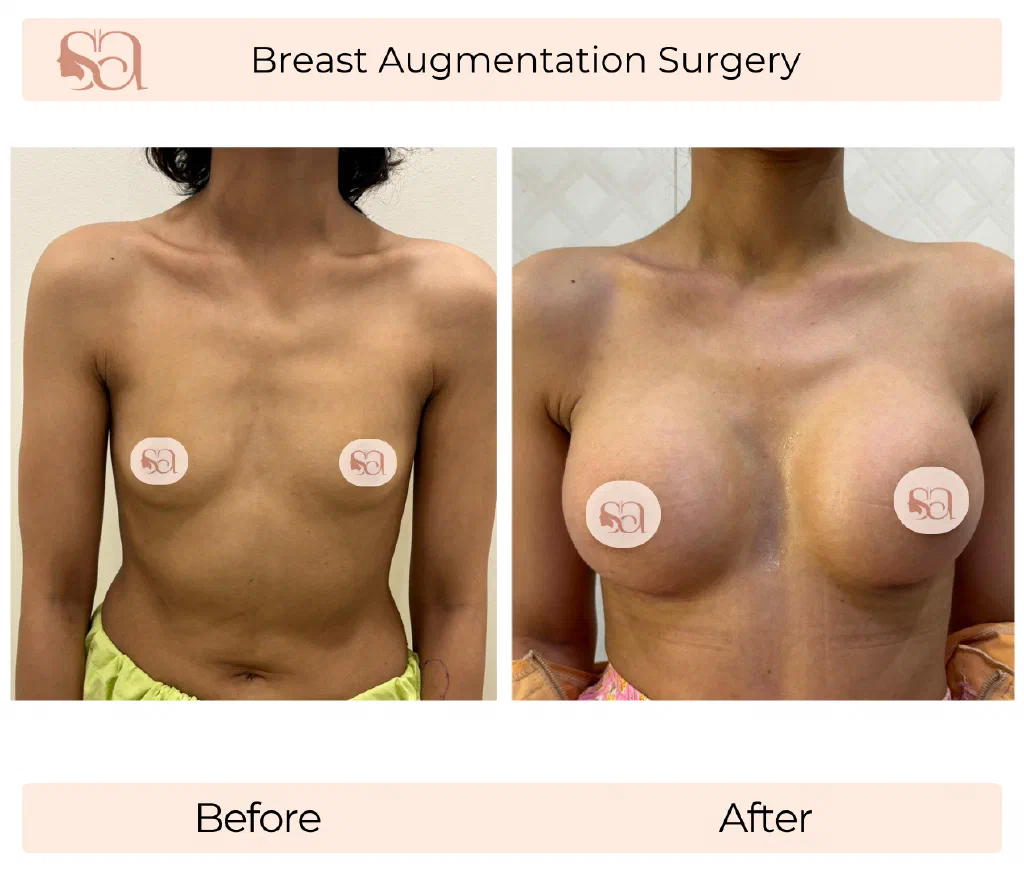
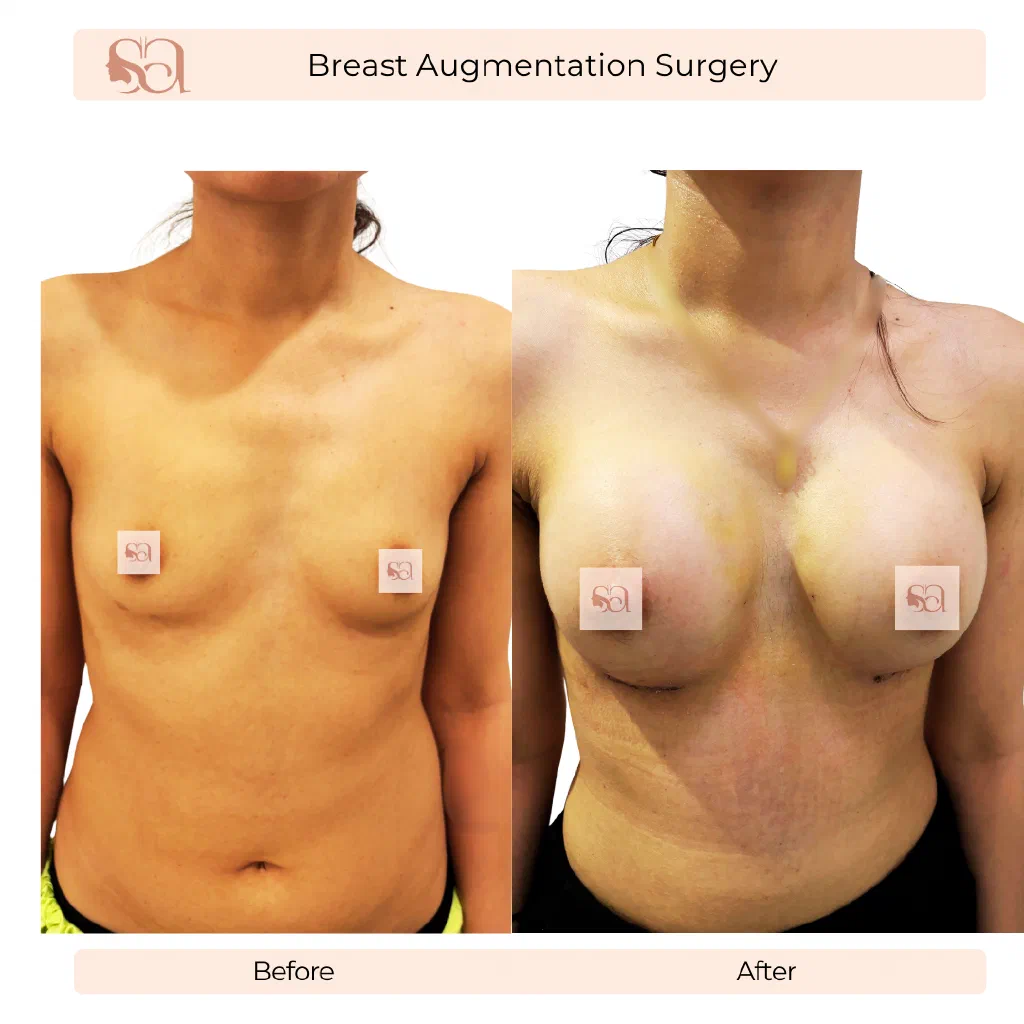
Breast augmentation is also not a route to a specific cup size. Cup labelling varies between bra brands and is a poor planning unit; volume in cubic centimetres of implant, placement, and the patient’s existing tissue together determine the post-operative shape. The size question is reframed at consultation in terms of chest width, tissue thickness, and the patient’s preference for proportionate-and-natural versus fuller-and-projected — a distinction Dr. Shikha walks through directly in the implant-sizing videos below.