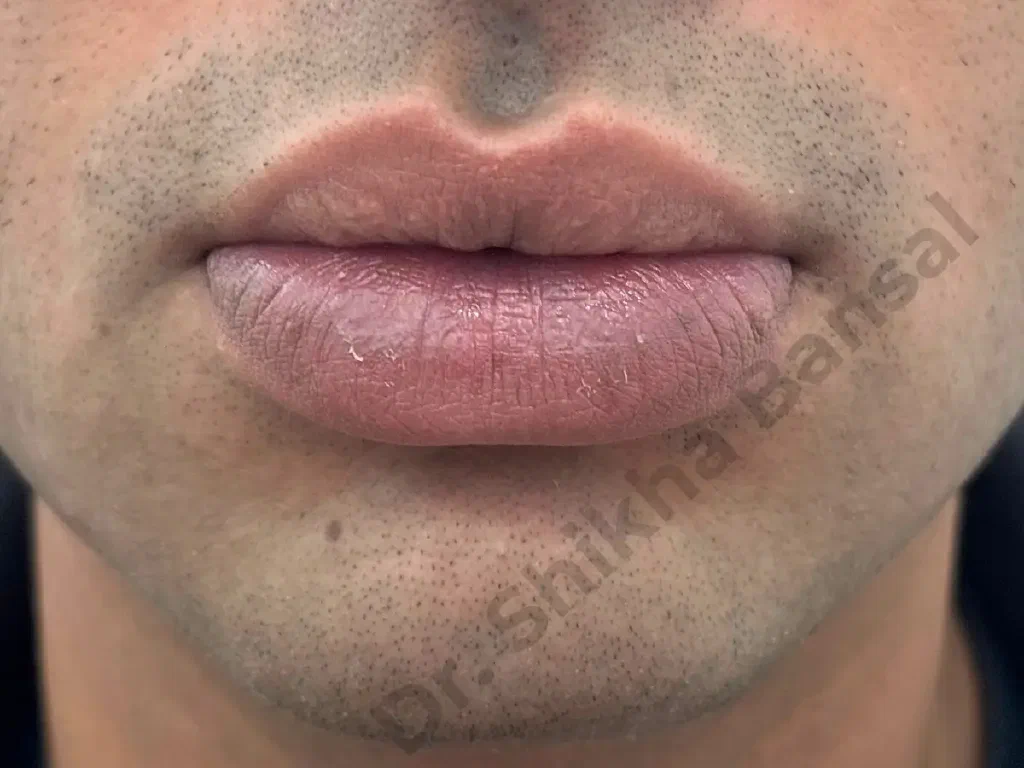
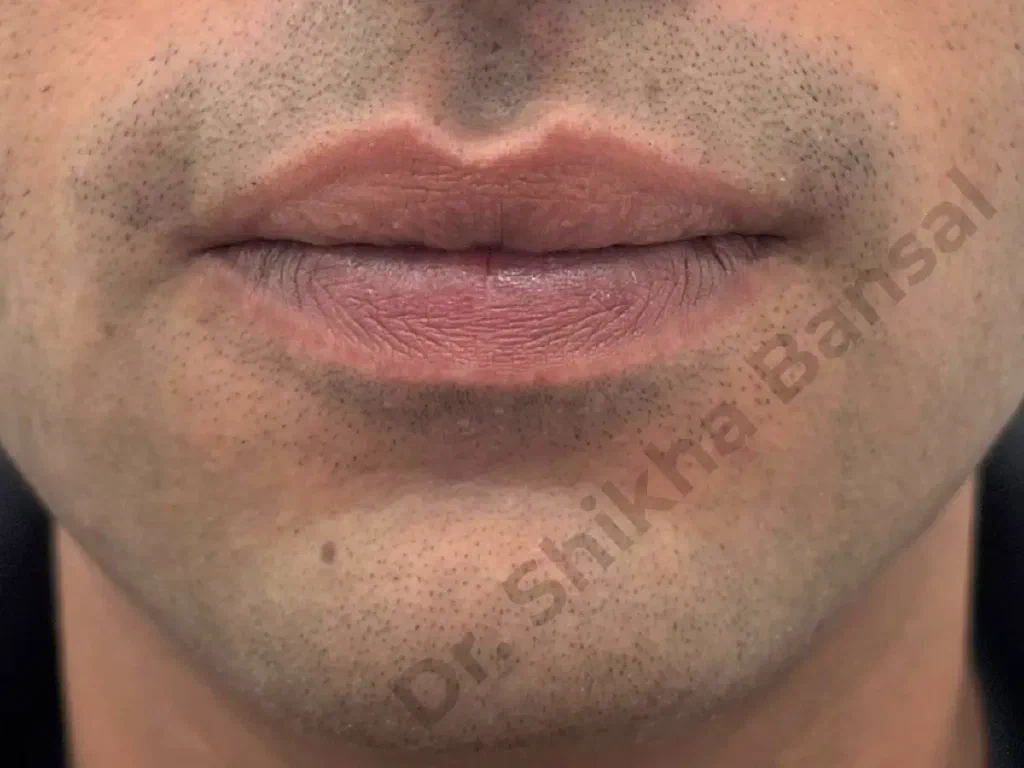
The visible part of the lip — the pink vermilion — is mostly mucosa stretched over the orbicularis oris muscle, with a thin layer of submucosa and minor salivary glands in between. How “full” a lip looks at rest is decided by three things: the height of the dry vermilion (the smooth pink strip), the bulk of the wet mucosa that everts forward at rest, and the resting tone of the orbicularis muscle behind it. Lip reduction works on the first two. It does not change muscle bulk, and it does not change the position of the upper-lip-to-nose distance (philtral height) or the chin-to-lip distance (mentolabial fold).
Genuine macrocheilia — a lip that is genuinely larger than the rest of the face would balance with — is most often constitutional and bilateral, more commonly affecting the lower lip than the upper, and is more frequent in patients of African or South Indian descent. A second large group is post-filler over-augmentation: the lip was filled, then re-filled, the hyaluronidase dissolved part but not all, and a residual fibrotic bulk remains that no further dissolution will remove. A third, smaller group is asymmetric fullness from previous trauma, mucocele, or healed haemangioma.
What lip reduction is not: it is not a treatment for “perceived” oversize where the lip is in fact within normal proportion. The first job at consultation is to measure the lip against the rest of the face — vermilion height, philtral length, lower-third proportion — and tell the patient honestly when the answer is no surgery rather than yes. Reduction that should not have been done is much harder to undo than not doing it in the first place.